SzPD: OVERT Vs. COVERT
SzPD: OVERT vs. COVERT
Salman Akhtar (a psychiatrist) provided a comprehensive phenomenological profile of Schizoid Personality Disorder in which classic and contemporary descriptive views are synthesized with psychoanalytic observations. This profile is summarized below and lists clinical features that involve six areas of psychosocial functioning and are organized by “overt” and “covert” manifestations. “Overt” and “covert” are not meant as different subtypes but as traits that may be present simultaneously within one single individual.
Self-concept - OVERT
compliant
stoic
noncompetitive
self-sufficient
lacking assertiveness
feeling inferior and an outsider in life
Self-concept – COVERT
cynical
inauthentic
depersonalized
alternately feeling empty, robot-like, and full of omnipotent, vengeful fantasies
hidden grandiosity
Interpersonal relations – OVERT
withdrawn
aloof
have few close friends
impervious to others’ emotions
afraid of intimacy
Interpersonal relations – COVERT
exquisitely sensitive [disambiguation needed]
deeply curious about others
hungry for love
envious of others’ spontaneity
intensely needy of involvement with others
capable of excitement with carefully selected intimates
Social adaptation – OVERT
prefer solitary occupational and recreational activities
marginal or eclectically sociable in groups
vulnerable to esoteric movements owing to a strong need to belong
tend to be lazy and indolent
Social adaptation – COVERT
lack clarity of goals
weak ethnic affiliation
usually capable of steady work
quite creative and may make unique and original contributions
capable of passionate endurance in certain spheres of interest
Love and sexuality – OVERT
asexual, sometimes celibate
free of romantic interests
averse to sexual gossip and innuendo
Love and sexuality – COVERT
secret voyeuristic interests
vulnerable to erotomania
tendency towards compulsive perversions
Ethics, standards and ideals – OVERT
idiosyncratic moral and political beliefs
tendency towards spiritual, mystical and para-psychological interests
Ethics, standards and ideals – COVERT
moral unevenness
occasionally strikingly amoral and vulnerable to odd crimes, at other times altruistically self-sacrificing
Cognitive style – OVERT
absent-minded
engrossed in fantasy
vague and stilted speech
alternations between eloquence and inarticulateness
Cognitive style – COVERT
autistic thinking
fluctuations between sharp contact with external reality and hyperreflectiveness about the self
autocentric use of language
More Posts from Muahahahahah and Others
Adhd things that need to be talked more about (because adhd is more than just not being able to focus)
Short term memory loss. Seriously, I forget things that are said to me 5 minutes ago or will forget I opened a soda and will have 3 open cans by the end of the day with none of them finished. A lot of people don’t know about this, and so they think that I don’t care enough to listen to what their saying (which I do!!! I just can’t remember it) or that I’m lazy because of all the things I don’t end up doing because I forgot I had to do them.
Lack of motivation. Listen, I honestly can’t do anything on my own for the most part. I have to have someone else tell me to do something or have them set goals for me because it’s so damn difficult for me to do it myself. Again, I’m not lazy, I just have trouble doing things on my own
Language processing difficulties. Sometimes, English and words in general don’t work out in my head. Reading or even listening to someone talk can be extremely difficult for me to understand because my brain just won’t work. Why? Can’t tell you 99% of the time! It’s not that I need to focus, it’s that my brain is just buffering.
Needing multiple forms of stimulation at all times. I have a tin of putty that I keep in my book bag and a smaller one I keep in my purse at all times because of this reason. If I want to learn anything at school, I have to be able to look at something, hear something, and have something to do with my hands. Otherwise, it’s probably a big nope for me. What’s frustrating is that since this isn’t talked about enough, I often get called childish or get looked down upon because I have to play with silly putty in a highschool class.
Hyperfixation. Adhd can mean not being able to focus, but it’s also focusing too much on something! This can mean anything from a certain interest someone is in to at that moment, to something like a song that has been stuck in your head for a week. People seem to not understand this and think that we’re boring and have nothing else to talk about or that we’re annoying because we keep bringing the same things up over and over again but that’s not the case. Trust me, I’m annoyed with the hit or miss song too, but at least it’s not playing in your head constantly like it is for me
These are all the ones I can think of right now, but it’s really important we talk about this stuff more. All of these things that come with adhd can be very frustrating for those around us because they don’t understand that we can’t help it. To an outsider, it may just look like a person with adhd is just lazy and doesn’t care, when it’s actually just how our brains are wired. None of us want to be frustrating to others!! In fact, all of this frustrates us too!! But since adhd is just known as “not being able to focus”, people don’t realize what all comes with it and how it can really fuck everyone over.
Please add more if you can think of anything else!! I’m horrible with lists lol
shoutout to abuse survivors & victims who fluctuate between “they didnt Really abuse me it wasnt That Bad its fine everything is okay” and “i hate them i want them to Burn” as a survival strategy, especially if you’re stil in regular contact with your abuser, and you wind up with a lot of self doubt because you spend so much time actively buying in to their gaslighting
it Is a survival strategy, it doesnt make you fake or bad.

Neuroscience of BPD
Lately I’ve been hearing that BPD isn’t a real mental illness because nothing is actually wrong with our brains and so, naturally, that means we’re using BPD as an excuse for our mood instability and impulsive behavior.
Guess what, naysayers? You were COMPLETELY right and totally called us out on our nefarious scheme!! We did, in fact, all convene at a super secret BPD convention of sorts and plotted to infiltrate the psychiatric field.
Haha, no. With the help of alix660 and porcelaindissonance I’ve learned a lot about the neuroscience behind BPD. And, while much more needs to be done in terms of BPD research, I did find strong evidence that BPD does have biological causes. You know. Just like an actual mental illness.
So here’s what we found, sorted by brain structure:
Amygdala: This brain structure is very heavily involved in emotional regulation and responses, particularly negative emotions. An fMRI study of BPD patients while being subjective to distressing visual stimuli found that our amydalas were significantly more reactive than those of control patients. This means that either the signals in our amgydalas are much more intense, or they continuing firing in our brains, preventing us from shutting down our emotional responses. Or perhaps it’s both, because that’s fun.
Another thing to note is that the amygdala receives tons of visual information, sent by the thalamus. The thalamus circumvents emotional processing in the prefrontal cortex (where we would consciously process how to regulate our emotions) and thus is involved in automatic, subconscious emotional processing. This is probably why our mood swings are so fast, unpredictable, and uncontrollable. It’s a knee-jerk reaction to even the tiniest triggers we come across. (Herpetz, et al.)
Amygdala volume is significantly reduced in BPD patients as well. (van Elst, et al.)
Hippocampus: This structure is involved in formation and retention of long-term memories, as well as autobiographical memories. Not only is hippocampal volume reduced in PTSD and MDD, it is also reduced in BPD. (van Elst, et al.)
I know from my studies that the reason for hippocampal volume reduction in PTSD and MDD comes from prolonged activation of the stress response. When we go into “fight or flight” mode, several physiological changes take place: our immune system shuts down, digestion stops, etc. But most importantly, when we enter “fight or flight,” glucose, which is necessary for cell metabolism, is redirected from the hippocampus and to your muscles. If you’re faced by a life-challenging thing, like a pack of velociraptors, you don’t want to think about it. You want to run, and you want to run fast. This is biologically adaptive in the short-term and in prey species… but not so with humans, because we can have this reaction to long-term, non-threatening stressors. So in long-term distress—like MDD, PTSD, and BPD—our hippocampus is starved of energy and atrophies. Result? We have absolutely terrible memory.
Prefrontal cortex: This is where we do our conscious thinking. More specifically, the medial prefrontal cortex, which is involved in processing emotional memories, is more active in the BPD brain. Essentially, this means we have difficulty mediating our conscious emotional responses.
In the ventrolateral prefrontal cortex, BPD brains also show abnormally high reactivity to aversive stimuli. This part of the cortex directly connects to our good friend the amygdala, and thus has some level of control over emotion-driven responses. (Herpetz, et al.)
In the anterior cingulate cortex, which is involved in feelings of apathy and emptiness, we see a significant reduction in volume in the BPD brain. The ACC is linked to self-harm and pain sensation. (van Elst, et al.)
In the orbitofrontal cortex, we also see volume reduction in BPD. The OFC is responsible for irritability, impulsivity, and instability, which are our favorite things.
Fusiform gyrus: Found in the temporal lobe, the fusiform gyrus is the facial recognition center of the brain. And—you guessed it—it’s also shown to be hyperactive in the BPD brain. Which makes sense when you think about it: we are EXTREMELY sensitive to even the slightest changes in the facial expressions of other people. If you appear disinterested, annoyed, angry, or otherwise upset, that’s an immediate trigger. (Herpetz, et al.)
Taken together, this means that the limbic circuits (emotional regulation) and the prefrontal cortex (executive control) are uniquely involved in BPD, resulting in a hyperarousal-dyscontrol syndrome. As of right now, no other psychiatric illness has this combination of reduced brain structure volumes and hyperactivity in certain regions. (van Elst, et al.)
Bonus!!!
Serotonin: Most of us know serotonin as a crucial neurotransmitter involved in major depressive disorder. But in BPD, studies show that reduced serotonin activity is found in several locations in the brain, including the cingulate cortex, which is critical in processing incoming emotional cues. Reduced serotonin impairs inhibition of aggressive behaviors, both directed at others (like outbursts) and directed at the self (like self-harm and self-hatred). Genes involved in serotonin can easily be studied. (Skodol, et al.)
Sources:
Skodol, et al. “The Borderline Diagnosis II: Biology, Genetics, and Clinical Course”
Herpetz, et al. “Evidence of Abnormal Amygdala Functioning in Borderline Personality Disorder: A Functional MRI Study”
van Elst, et al. “Frontolimbic Brain Abnormalities in Patients with Borderline Personality Disorder: A Volumetric Magnetic Resonance Imaging Study”
PS I did read several other articles that corroborated these findings, so it’s not like these are the only sources of evidence I found that point to the biological nature of BPD.
it would've been better for everyone if I had stopped having a heartbeat years ago






Chernobyl (2019) Episode 1 dir. Johan Renck “What is the cost of lies? It’s not that we’ll mistake them for the truth. The real danger is that if we hear enough lies, then we no longer recognise the truth at all.”
... Pls cute girls and boys... Tag your cuteness right with #cute rather than #cut...
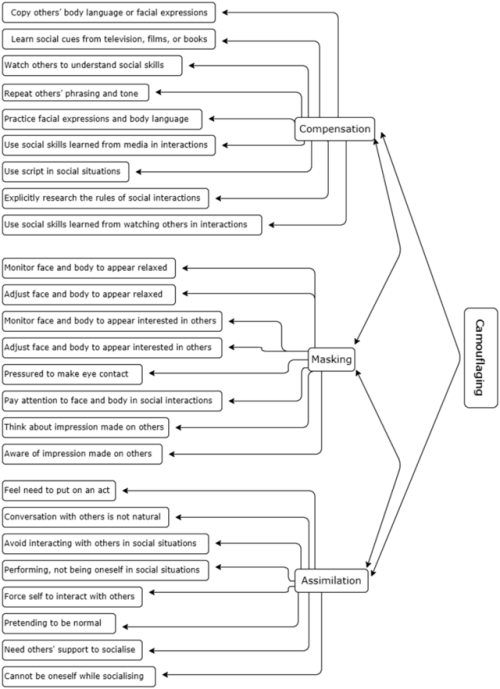
[ID: Image depicting three types of camouflaging - compensation, masking, and assimilation. Under compensation it lists - coping others’ body language and facial expressions, learn social cues from television/films/or books, watch others to understand social skills, repeat others’ phrasing and tone, practice facial expressions and body language, use social skills learned from media in interactions, use script in social situations, explicitly research the rules of social interactions, and use social skills learned from watching others in interactions. Under masking it lists - monitor face and body to appear relaxed, adjust face and body to appear relaxed, monitor face and body to appear interested in others, adjust face and body to appear interested in others, pressured to make eye contact, pay attention to face and body in social interactions, think about impression made on others, and aware of impression made on others. Under assimilation it lists - feel need to put on an act, conversation with others is not nature, avoid interacting with others in social situations, performing/not being oneself in social situations, force self to interact with others, pretending to be normal, need others’ support to socialize, and cannot be oneself while socializing./]
Image provided from https://link.springer.com/article/10.1007%2Fs10803-018-3792-6. Entitled “Social Camouflaging Model.”

- Hello, good morning! How did you sleep?
- Oh, hi! I didn't sleep!
💖
-
 i-darkling liked this · 2 years ago
i-darkling liked this · 2 years ago -
 gerome-inanity liked this · 2 years ago
gerome-inanity liked this · 2 years ago -
 braxnfog liked this · 2 years ago
braxnfog liked this · 2 years ago -
 julichris liked this · 2 years ago
julichris liked this · 2 years ago -
 lucky-snoodle liked this · 3 years ago
lucky-snoodle liked this · 3 years ago -
 who-are-we-to-change liked this · 3 years ago
who-are-we-to-change liked this · 3 years ago -
 littleboybeep liked this · 4 years ago
littleboybeep liked this · 4 years ago -
 cuntdracula99 liked this · 4 years ago
cuntdracula99 liked this · 4 years ago -
 15514000 liked this · 4 years ago
15514000 liked this · 4 years ago -
 fendyvent reblogged this · 5 years ago
fendyvent reblogged this · 5 years ago -
 geryuganshupu liked this · 5 years ago
geryuganshupu liked this · 5 years ago -
 jarofteeth liked this · 5 years ago
jarofteeth liked this · 5 years ago -
 thoughtfullyscentedgarden liked this · 5 years ago
thoughtfullyscentedgarden liked this · 5 years ago -
 the-wretched-automatons liked this · 5 years ago
the-wretched-automatons liked this · 5 years ago -
 cristallineclearvibesonly liked this · 5 years ago
cristallineclearvibesonly liked this · 5 years ago -
 bpdealingwithit reblogged this · 5 years ago
bpdealingwithit reblogged this · 5 years ago -
 watanuki liked this · 5 years ago
watanuki liked this · 5 years ago -
 cupcakesunlimited reblogged this · 5 years ago
cupcakesunlimited reblogged this · 5 years ago -
 nebulaboy liked this · 5 years ago
nebulaboy liked this · 5 years ago -
 yourselfcola reblogged this · 5 years ago
yourselfcola reblogged this · 5 years ago -
 grumpyone3 liked this · 5 years ago
grumpyone3 liked this · 5 years ago -
 br-ead-loaf liked this · 5 years ago
br-ead-loaf liked this · 5 years ago -
cupcakesunlimited reblogged this · 5 years ago
-
 muahahahahah reblogged this · 5 years ago
muahahahahah reblogged this · 5 years ago -
 schizoidrats reblogged this · 5 years ago
schizoidrats reblogged this · 5 years ago -
 creaturecorpse liked this · 5 years ago
creaturecorpse liked this · 5 years ago -
 yupori liked this · 5 years ago
yupori liked this · 5 years ago